619
Views & Citations10
Likes & Shares
Nigeria is currently facing a rapid and widespread
increase in human immunodeficiency virus (HIV)/acquired immunodeficiency
syndrome (AIDS). The activities of female sex workers (FSWs) have contributed
to the mounting epidemic of HIV/AIDS and other sexually transmitted diseases
(STDs). Therefore, this study aimed to assess the knowledge sexually
transmitted infection (HIV/AIDS) among female sex worker in Sokoto. A
cross-sectional form of descriptive survey research design was used for this
study. Data obtained for the study was collected from 100 (one hundred) females
sex worker with structured questionnaire in two sections A and B. Section A,
was made up of three questions on demographic data (age, level of education and
year of prostitute). Section B, contained twelve (12) questions on knowledge of
sexually transmitted infection (HIV/AIDS). Chi-square (χ2) 732.4829
is greater than the critical value 55.758, df=40, there is a statistically
significant relationship between the age of female sex worker and the knowledge
of HIIV/AIDS. Chi-square (χ2) 775.09 is greater than the critical
value 55.758, df=40 there is a statistically significant relationship between
the educational level of female sex worker and the knowledge of HIIV/AIDS.
Chi-square (χ2) 1338.669 is greater than the critical value 55.758,
df=40 there is a statistically significant relationship between the years of
been a female sex worker and the knowledge of HIIV/AIDS rejection the null
hypothesis. This study showed that female sex worker in this study area,
possessed very good knowledge of sexually transmitted infection (HIV/AIDS).
Keywords: Sexually transmitted
infection/diseases, HIV/AIDS, Age, Knowledge, Female sex workers (FSWs),
Educational level
INTRODUCTION
Sex worker is a
person who is employed in the sex industry [1]. The term is used in reference
to all those in all areas of the sex industry including those who provide
direct sexual services as well as the staff and management of such industries
[1]. Some sex workers are paid to engage in sex acts or sexually explicit
behavior which involve varying degrees of physical contact with clients
(prostitutes and some but not all professional dominants); pornography models and actors engage
in sexually explicit
behavior
Statement of problem
HIV infection among women in the United
States decreased from 9.5 per 100,000 persons in 2008 [2], to 6.1 per 100,000
in 2014 [3]. However, there may be subgroups among the female population where
HIV transmission remains high, such as female sex workers. Globally, sex
workers are among the populations most affected by HIV. A systematic review of
HIV infection among female sex workers in developing countries found an overall
prevalence of 11.8% (95% confidence interval (CI) 11.6-12.0), a level that is
significantly greater than in the general female population (Odds Ratio: 13.5
(95% CI 10.0-18.1)) [11]. A recent update to this systematic review included
additional data from 2011 to 2013 and showed that the estimated prevalence
varied widely by region from 0.3% (95% CI 0.1-0.8) in the Middle East and North
Africa to 29.3% (95% CI 25.0-33.8) in Sub-Saharan Africa.
AIMS AND OBJECTIVES
The main purpose of the study was to
determine the behavioral practices promoting malaria drug resistance among
adults in Sokoto metropolis. In specific terms, the objectives of the study
include:
1. To
determine the influence of age on the Knowledge of sexually transmitted
infection (HIV/AIDS) among female sex worker in Sokoto metropolis.
2. To
ascertain the influence of level of education on Knowledge of sexually
transmitted infection (HIV/AIDS) among female sex worker in Sokoto metropolis.
SIGNIFICANCE OF THE
STUDY
Results of the study would reveal Knowledge
of sexually transmitted infection (HIV/AIDS) among female sex worker in Sokoto
metropolis. Specifically, result of the study would be significant to adults
(male/female), Public health officers, health counselors, health educators,
curriculum planners, medical allied personnel and researchers in assessing
Knowledge of sexually transmitted infection (HIV/AIDS) among female sex worker
in Sokoto metropolis. Although good knowledge, assessment would motivate
effectiveness of program in this locality. Results of the study would motivate
public health workers toward identifying behavioral practices (risk factors)
that are common in this locality. Health counselors would through the results
of this study develops and adapts effective method on the best malaria
preventive practices. Health educators, curriculum planners and researchers
would be able to identify gaps in Knowledge of sexually transmitted infection
(HIV/AIDS) among female sex worker in Sokoto that can aid in the development of
health education and health promotion concepts that can be utilized in the
community to address the deficiencies.
RESEARCH QUESTIONS
The following research questions gave
direction to the study:
1. What
is the level of influence of age on the Knowledge of sexually transmitted
infection (HIV/AIDS) among female sex worker in Sokoto metropolis?
2. What
is the influence of level of education and year of female sex work on Knowledge
of sexually transmitted infection (HIV/AIDS) among female sex worker in Sokoto?
HYPOTHESES
The following null hypotheses were postulated
for the study
1. There
is no significant difference in the age on the Knowledge of sexually
transmitted infection (HIV/AIDS) among female sex worker in Sokoto metropolis.
2. There
is no significant difference on level education and year of female sex work on
Knowledge of sexually transmitted infection (HIV/AIDS) among female sex worker
in Sokoto metropolis.
RESEARCH DESIGN
A cross-sectional form of descriptive survey
research design was used for this study. This is because descriptive studies
are used when the characteristics of a population are either unknown or
partially known; this justified the use of similar design in a study of similar
nature.
Study area
Sokoto is one of the seven states that form
the North West geopolitical zone of Nigeria. It is bordered to the north by the
Republic of Niger, Zamfara State to the east, Kebbi state to the south and
west. It is situated in the savannah on the temperature of 44 degree Celsius
annually. The city of Sokoto is its capital. Sokoto state traces its origin to
the Sokoto Caliphate founded in 1809 by Shehu Usmandan Fodio, the leader of the
jihadists who overthrew the Hausa state of Gobir, Kano, Katsina and
Kanem-Bornu. The empire fell after the British conquest of 1903 and the death
of Attahiru, the Sultan of Sokoto and became part of the Northern Region in the
three-region structure of 1954. In 1967, Nigeria, the military administration
of General Yakubu Gowon merged Sokoto and Niger provinces to form the North
Western state. In 1976, North Western State was spilt into Sokoto and Niger
states by the military administration of General Murtala Muhammed. Sokoto State
covers an area of 28,232.37 km2. The state is located between
latitudes 40 to 60 north and longitudes 110 to 130 east has a population of
3,702,676 (2006 census figures). It accounts for 2.3 percent of Nigeria’s total
population. Prior to the establishment of Sokoto as a ribat (military camp or
frontier) in 1809, the area that is modern-day Sokoto state was home to Hausa
state with large populations. These states eventually fell under the control of
UsmandanFodio and the Fulani jihadists and became part of the Sokoto Caliphate.
In 1817 when Usman died, his son Muhammed Bello succeeded him as the Sultan of
Sokoto. Usman’s brother Abdullahi was given the western divisions of the
caliphate to run; however, supreme authority rested with Bello. At the height
of its power, the Sokoto Caliphate extended as far as Ilorin (in modern-day
Kwara State). The Hausa are the largest ethnic group in Sokoto State while the
Fulani are its second largest. Minority include the Zabarmawa, Tuareg and the
Dakarkari. The majority of the population is Sunni Muslim. There is a small
Shia minority. There are twenty-three local government areas (LGAs) in Sokoto.
Each has a chairman as its administrative head. The Islamic community in
Nigeria considers the person of the Sultan as ‘First among Equals’. He is both
the political head of the Fulani as well as the supreme spiritual head of the
rough 70 million Muslims in Nigeria. Currently occupying the site is Sultan
MuhammaduSa’ad Abubakar III, the 20th sultan of Sokoto. Agriculture
is the mainstay of Sokoto’s economy. The riverine floodplains produce cash
crops, including peanuts (groundnuts), cotton and rice. Sorghum, millet,
cowpeas and cassava are grown in the upland areas. Much of the land in the
state is used for grazing cattle. Cattle hides, goatskin, sheepskins and
finished leather products are significant exports, as are cattle, goats and
fowl. The state possesses limestone and kaolin deposits and Sokoto City, the
state capital, is home to a cement factory, tanneries and a modern abattoir.
Festivals include Kalankuwa, Halbi, Sharo, AikinGawa, Shan Gumba-Pap drinking
and Remo Fishing Festival.
Method of data
collection
A letter of introduction (Appendix D) signed by the Head of Department of Public Health Imo
State University, Owerri was presented to the district head of Kwannawa area to
allow entry for data collection. Two (2) trained research assistants were
involved in explaining to the respondents on face to face basis detail of what
the research is meant for.
Population of the
study
The accessible population of the study
consisted of an estimated one thousand (1,000) adults (female) (18-70 years) in
Kwanawa area.
Sample/sampling
technique
The sample for the study consisted of 100
(one hundred) adults’ females randomly drawn areas in Kwannawa area. Ten
percentage (10%) of the accessible population was used as sample size, Nwana
(2011) opined that if the population is in few thousand 10% will be appropriate
as the sample size.
Instrument for data
collection
The main instrument for data collection
consisted of structured questionnaire. The structured questionnaire was in two
sections A and B. Section A, was made up of three questions on demographic data
(age, level of education and year of prostitute). Section B, contained nine (9)
questions on Knowledge of sexually transmitted infection (HIV/AIDS) among
female sex worker.
Scope of the study
The study was delimited to the Knowledge of
sexually transmitted infection (HIV/AIDS) among female sex worker (18-70 years)
in Sokoto metropolis. It was delimited to independent variables of age, female
sex worker and levels of education. It was further delimited to adult’s female
sex worker (18-70 years) in Kwanawa area Sokoto metropolis. It involved young
adult age (18-40), middle adult (41-65) and older adult above 65 years. It was
delimited to the use of structured questionnaire as the main instrument for
data collection. Finally it was delimited to the use of descriptive statistic
of frequency and percentage as well as inferential statistic of chi square at
0.05 level of significant for data analysis.
Method of data
analysis
Data collected were analyzed using
descriptive statistic of frequency count, normative percentage and grand mean;
as well as inferential statistics of chi-square (χ2). The level of
significant was fixed at 0.05. Appropriate degrees of freedom were worked out.
Data presentation
and analysis
The chapter deals with data presentation,
analysis and discussion of the results obtained based on the objectives, and
the research questions of the study as well as the hypotheses. Research
questions were answered using percentages (%); null hypotheses were tested
using inferential statistics of chi-square. The level of significance was set
at 0.05.
RESULTS AND DISCUSSION
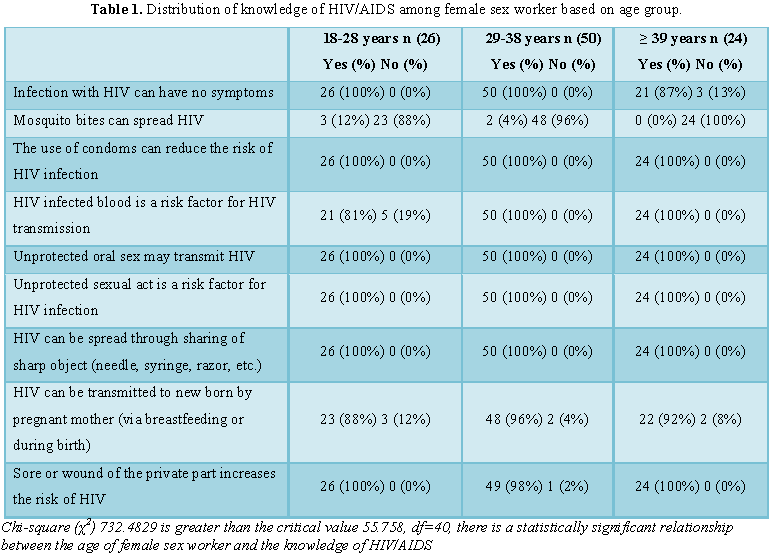
The influence
of age of female sex worker on the of knowledge of sexually transmitted
infection (HIV/AIDS) showed that among subjects of different age group 18-28
years, 29-38 years and ≥ 39 years, 26 (100%), 50 (100%) and 21 (87%) answered
yes correctly respectively that HIV infections has no symptoms. 23 (88%), 48
(96%) and 24 (100%) answered No correctly that mosquito bite does not spread
HIV across different age group 18-28 years, 29-38 years and ≥ 39 years,
respectively. There were overwhelming (100%) yes correctly that the use of
condoms can reduce the risk of HIV infection across different age group 18-28
years, 29-38 years and ≥ 39 years, respectively. HIV infected blood is a risk
factor for HIV transmission 21 (81%) answered yes correctly in 18-28 years and
100% yes each for 29-38 years and ≥ 39 years, respectively. There is a general
100% yes correctly that Unprotected oral sex may transmit HIV, Unprotected
sexual act is a risk factor for HIV infection and HIV can be spread through
sharing of sharp object (needle, syringe, razor, etc.) respectively different
age group 18-28 years, 29-38 years and ≥ 39 years. 23 (88%), 48 (96%) and 22
(92%) answered yes correctly across different age group 18-28 years, 29-38
years and ≥ 39 years, respectively, that HIV can be transmitted to new born by
pregnant mother (via breastfeeding or during birth). 26 (100%), 49 (98%) and 24
(100%) answered yes correctly across different age group 18-28 years, 29-38
years and ≥ 39 years, respectively that present of sore or wound on the private
part increases the risk of HIV. Chi-square (χ2) 732.4829 is greater
than the critical value 55.758, df=40, there is a statistically significant
relationship between the age of female sex worker and the knowledge of
HIIV/AIDS (Table 1).
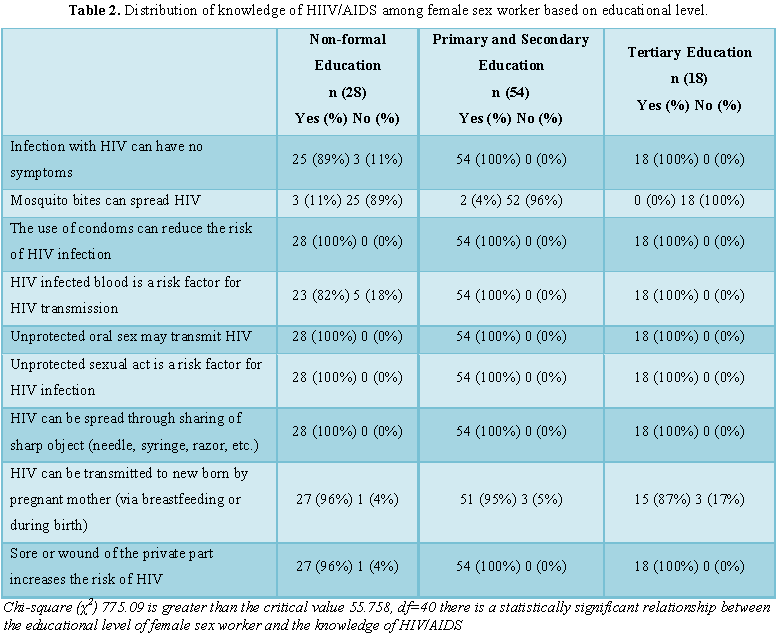
The influence of educational level of female sexual worker on the knowledge of sexually transmitted infection (HIV/AIDS), showed that 25 (89%), 54 (100%) and 18 (100%) answered yes that HIV infection those not have symptoms across Non formal education level, primary and secondary educational level and tertiary educational level subjects respectively. On mosquito bite spreading HIV, 25 (89%), 52 (96%) and 18 (100%) answered No correctly that mosquito bite does not spread HIV across non-formal education level, primary and secondary educational level and tertiary educational level subjects, respectively. Among subjects there were 100% yes across non-formal education level, primary and secondary educational level and tertiary educational level subjects respectively that the use of condoms can reduce the risk of HIV infection. On HIV infected blood been a risk for HIV infection 23 (82%), 54 (100%) and 18 (100%) answered yes correctly across Non formal education level, primary and secondary educational level and tertiary educational level subjects, respectively. Across non-formal education level, primary and secondary educational level and tertiary educational level subjects there were 100% yes correctly that unprotected oral sex may transmit HIV; unprotected sexual act is a risk factor for HIV infection same for HIV can be spread through sharing of sharp object (needle, syringe, razor). 26 (96%), 51 (95%) and 15 (87%) answered yes correctly across Non formal education level, primary and secondary educational level and tertiary educational level subjects respectively that HIV can be transmitted to new born by pregnant mother (via breastfeeding or during birth). 27 (96%), 54 (100%) and 18 (100%) answered yes correctly across Non formal education level, primary and secondary educational level and tertiary educational level subjects respectively that present of Sore or wound on the private part increases the risk of HIV. Chi-square (χ2) 775.09 is greater than the critical value 55.758, df=40 there is a statistically significant relationship between the educational level of female sex worker and the knowledge of HIIV/AIDS (Table 2).
CONCLUSION
This study
showed that female sex worker in this study area, possessed very good knowledge
of sexually transmitted infection (HIV/AIDS).
1. Baptie
T (2009) Sex worker? Never met one! Sisyphe.org. Retrieved 2009-09-12.
2. CDC
(2013) Diagnosis of HIV infection in the United States and dependent areas,
2011. HIV Surveillance Report 23: 84.
3. CDC
(2015) Diagnoses of HIV Infection in the United States and Dependent Areas,
2014. Atlanta, GA.
4. Burnes
TR (2017) Sex work. Thousand Oaks: Sage Publications, Inc.
5. Farley
M (2006) Prostitution, trafficking, and cultural amnesia: What we must not know
in order to keep the business of sexual exploitation running smoothly. Yale
Journal of Law and Feminism 18: 109-144.
6. Harcourt
C, Donovan B (2005) The many faces of sex work. Sex Transm Infect 81: 201-206.
7. Givetash
L (2017) Some sex workers choose industry due to benefits of occupation: Study.
The Globe and Mail. Toronto: Phillip Crawley.
8. Breslin
S (2011) Why do women become sex workers and why do men go to them? The Guardian.
UK.
9. Weitzer
R (2000) Sex for sale: Prostitution, pornography and the sex industry. New
York: Routledge Press.
10. Rusakova
M, Rakhmetova A, Strathdee SA (2015) Why are sex workers who use substances at
risk for HIV. Lancet 385: 211-212.
11. Baral
S, Beyrer C, Muessig K, Poteat T, Wirtz AL, et al. (2012) Burden of HIV among
female sex workers in low-income and middle-income countries: A systematic
review and meta-analysis. Lancet Infect Dis 12: 538-549.
12. de
Araújo Patrício ACF, Bezerra VP, Camargo BV, de Almeida Nogueira J, Moreira
MASP, et al. (2016). Knowledge of women sex workers about HIV/AIDS. Int Arch
Med 9: 22-36.
13. Ryan
C, Kinder R (1996) Sex, tourism and sex tourism: Fulfilling similar needs?
Tourism Management 17: 507-518.
-
 Table 1
Table 1 -
Table 2
-
Table 3